Bilious Vomiting in Neonates
A cornerstone of neonatal practice is the concept that green vomiting is indicative of mechanical obstruction until proven otherwise. None the less not all bilious vomiting has a surgical cause. Stringer et al. (2002) report no mechanical obstruction in as many as 62% patients, whilst Mohinudden et al. (2015) found 54% of term babies referred with bilious vomiting had no surgical cause. So how do we decide? Are there sensitive or specific findings on clinical examination, blood tests or imaging? There are no easy answers, it appears, as Mohinidden’s study (2015) demonstrated that clinical signs and x-ray findings did not consistently differ between those babies with time-critical causes for surgical pathology and those without. Borooah et al. (2010) determined “clinical examination and plain abdominal films had little to no predictive value in diagnosing midgut volvulus” though upper GI contrast with or without ultrasound “improved the predictive value in diagnosing surgical pathology”.
Clinical signs and findings on imaging are frequently non-specific therefore. What is worse is that a late or undiagnosed malrotation volvulus can rapidly progress to irreversible necrosis potentially of the entire bowel. With such significant morbidity and indeed mortality at stake all babies with bilious vomiting must undergo surgical review unless a clear alternative cause is found.
Ultimately the main imaging modality of choice is an upper GI contrast to exclude malrotation volvulus. The associated costs in terms of transport, time and effort in managing such babies is therefore substantial as frequently local hospitals do not have this facility close to hand and require paediatric surgical expertise for ongoing assessment and management. Whilst this surgical stance is unambiguous, neonatal practice however appears not to be so clear cut. In a survey of neonatologist 80% of respondents said they would simply admit a baby with bilious vomiting for observation (Walker et al. 2007). 50% did not consider a contrast study to be a first line investigation whilst one third of neonatologist felt surgical referral was not appropriate for a baby following a single bilious vomit. Whilst data is incomplete and opinion on management is divided, prioritisation and urgent referral of these neonates for surgical opinion is uncontroversial. Given the diagnostic challenges a low index of suspicion is warranted and a systematic approach to the exclusion of pathology should be then be undertaken.
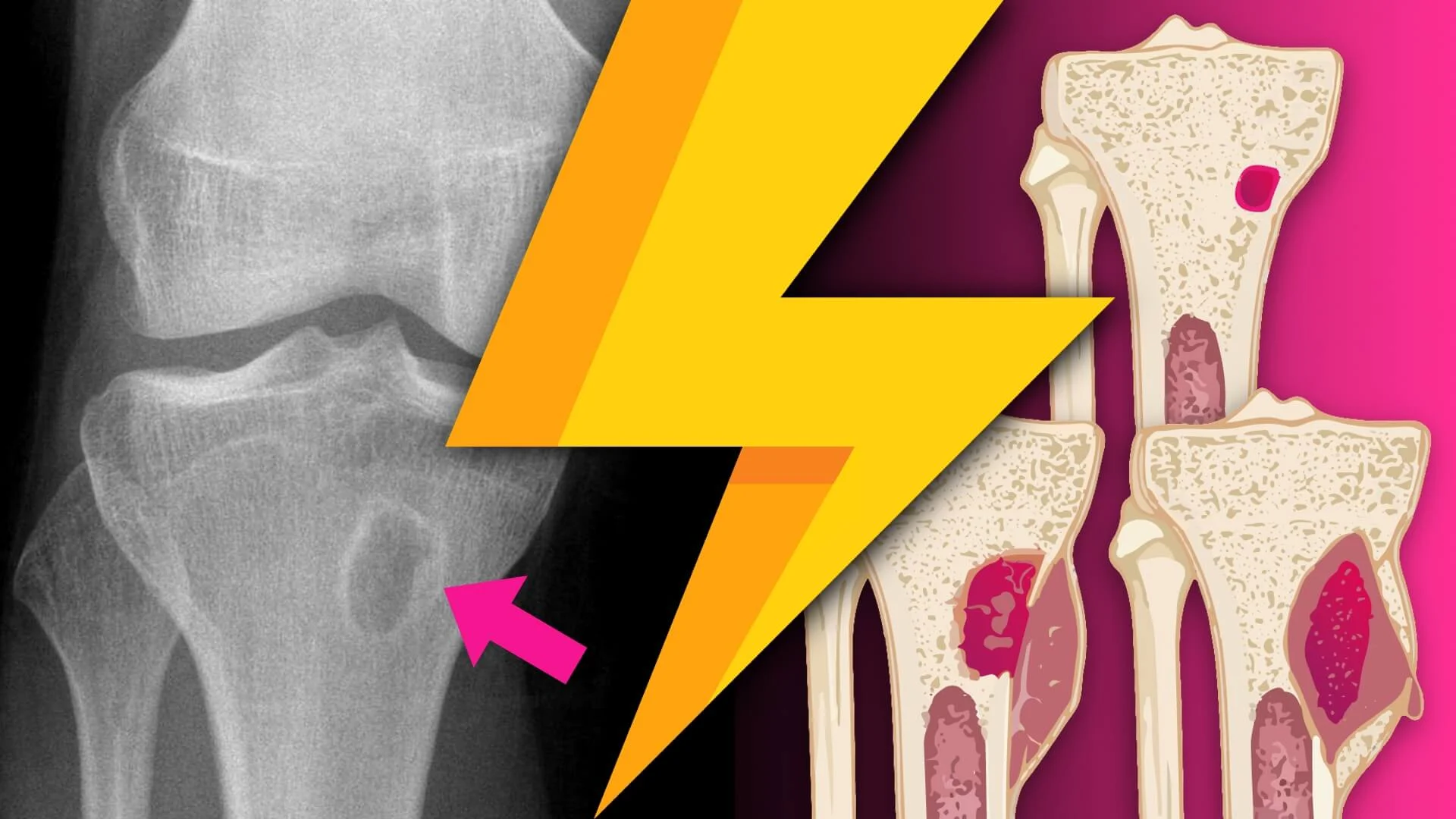
Important causes of intestinal bilious vomiting (including obstruction)
Duodenal atresia
Malrotation and volvulus
Jejunoileal atresia
Meconium ileus
Meconium plug syndrome
Necrotising enterocolitis
For further discussion of these pathologies, see the following articles…
References
- Godbole P, Stringer MD, Bilious vomiting in the newborn: how often is it pathologic? J Pediatr Surg 2002;37:909–11.
- Mohinuddin S, Sakhuja P, Bermundo B, et al. Outcomes of full-term infants with bilious vomiting: observational study of a retrieved cohort. Arch Dis Child 2015;100:14–17.
- Borooah M, Narang G, Mishra A, et al, Bilious vomiting in the newborn period: surgical incidence and diagnostic challenges. Archives of Disease in Childhood 2010;95:A86.
- Walker GM, Raine PM, Bilious vomiting in the newborn: how often is further investigation undertaken? J Pediatr Surg 2007;42:714–16.
- Kumar N, Curry JI, Bile-stained vomiting in the infant: green is not good! Archives of Disease in Childhood - Education and Practice 2008;93:84-86.
- Kimura K, Loening-Baucke V. Bilious vomiting in the newborn: rapid diagnosis of intestinal obstruction. American Family Physician 2000;61(9):2791e8.